For the first time (to my knowledge), the editorial staff of the New York Times has acknowledged that there is a PHYSICIAN SHORTAGE and pointed to the need to increase the number of residents being trained, not that I didn’t try to tell them. Since 2002, when it was clear to me and my colleagues that the US was headed for exactly the kind of shortages that are now unfolding, I sent them three OpEds and two letters explaining the problem. They chose to ignore all of them and, instead, relentlessly pursue the Dartmouth-inspired dogma that the system was fraught with waste and inefficiency and, therefore, needed fewer, not more, doctors. David Leonhart, the Times economics columnist, even awarded his 2007 Book-of-the-Year Award to “Overtreated” which was written by Shannon Brownlee, a publicist for the Dartmouth group.
The first mention in the Times that a doctor shortage was in the works appeared in a front page article by Annie Lowrey and Robert Pear on July 12, 2013, accurately entitled “Doctor Shortage Likely to Worsen With Health Law.” Eighteen months later, the Times reversed course through an OpEd by one of its regulars, Ezekiel Emanuel, together with Scott Gottlieb, a fellow of the American Enterprise Institute, entitled “No, There Won’t Be a Physician Shortage,” which called for greater productivity of physicians rather than a greater supply of them. And now, at long last, prompted by the physician shortage at the VA (which needs 1,500 more), the Times admits that there aren’t enough and that there won’t be enough and, therefore, the US had better train more. Thank you, New York Times!
Since they chose to ignore the problem for more than a decade and chose not to print my missives, I have reproduced them below. At a minimum, they are historically interesting You may also wish to read a paper I published in the Nov. 13, 2013 issue of JAMA, entitled “Unraveling the Physician Supply Dilemma.”
WHO WILL FIGHT THE BATTLE FOR BETTER HEALTH?February 2002
Last month, President Bush unveiled his health care agenda before an enthusiastic crowd at the Medical College of Wisconsin. He prefaced his comments with remarks about the war on terrorism and about the soldiers who are fighting that war, and he described its ideological basis —patriotism and love of freedom—qualities that, he noted, both parties admired. But his purpose was to discuss another war—the battle for a better health care system, a battle whose strategy rests on a different ideological base—compassionate conservatism. Compassionate because it offers “health credits” and other ways to assure health insurance for everyone, but conservative because the range of basic benefits will be tied to one’s ability to pay. Compassionate because it will include prescription benefits and research support for developing tomorrows therapeutics, but conservative because it will place a veil over areas of research that are abhorrent to the right. Compassionate because everyone will have catastrophic health insurance of comparable value, but conservative because it is another step along the road from defined benefits to defined contributions.
There is more to learn, and debate is certain to be vigorous, but President Bush has restarted a process that has been dormant since the disappointing experience of the Clinton Health Plan. Yet, as I sat listening to his broad agenda—his strategy for this other war—and as I heard him compliment the students who were present and tell them how, freed of the burdens of litigation and regulation, they would be better able to deliver quality care, I was struck by the realization that it won’t happen; that, unlike the military preparedness for the war on terrorism, there won’t be enough soldiers for the war for better health; that at a time when the President speaks about better access to specialists and more research to give them the tools that they now lack, patients are waiting ever longer to see a doctor.
Based on economic and demographic trends, my colleagues and I have projected that this situation will progressively worsen. Without adequate numbers of physicians, the dreams of more expansive and accessible health care simply cannot materialize. It takes a day to pass a prescription drug benefit. It takes a decade to train a doctor. If we want to have enough physicians to fight the President’s other war, we had better start educating more of them now.
WHO WILL BE TOMORROW’S DOCTORS? June 2006
Headlines announce an epidemic of obesity. Wal-Mart is coerced into providing broader health insurance. The growing numbers of uninsured is a national disgrace. More health care is wanted, and more will be needed. Costs are a problem, but a way will be found to pay for it. The question is, “who will provide it?”
Readers of the Times know full well that there’s a major nursing shortage. What’s less well appreciated is that there’s a looming physician shortage. Based on long-term economic and demographic trends, my colleagues and I have estimated that the US will need an additional 200,000 physicians over the next 15-20 years. That will require an increase in the number of doctors being trained annually from about 25,000 to 35,000 – a 40% increase. Moreover, because the lead-time to start new schools, educate doctors and allow them to complete residency training is so long, few of these additional physicians will be enter practice for a decade or more, even if a maximal effort were undertaken today. Yet, little effort is underway to expand medical school capacity, and no real effort is being made to increase the number of residency positions, which were capped by Medicare at their 1996 levels.
It’s not that the problem is out of view. Medical societies in Massachusetts, Wisconsin, California and ten other states have published reports with titles such as “And Then There Were None: The Coming Physician Supply Problem” and “Who Will Care for Our Patients?” Merritt, Hawkins & Associates, the nation’s largest physician recruitment firm, published a book entitled “Will The Last Physician In America Please Turn Off The Lights? A Look at America’s Looming Doctor Shortage.” And similar levels of alarm have emanated from associations of cardiologists, radiologists, anesthesiologists, pulmonary-critical care physicians and a dozen other specialties.
Despite this, most policy-makers have remained on the sidelines. One reason is a lingering concern that the forecasts of shortages could be wrong. Another is a long-standing belief that it’s better to undershoot than to train too many physicians. Too many could fuel more health care spending, so they believe — any deficiencies can be filled from other countries. But the US has relied so heavily on other countries that 25% of our current physicians are foreign trained, principally from developing countries. Taking still more could bring the health care systems of many of these countries to the brink of collapse.
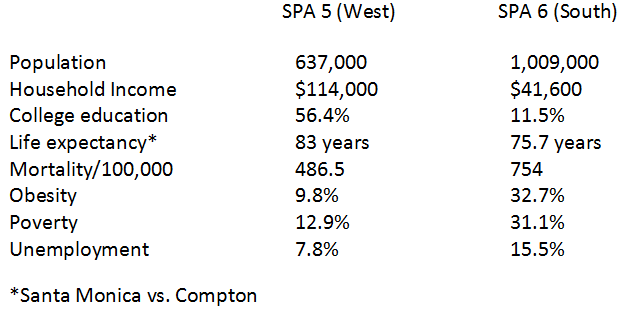
Now the landscape is sullied by the statistical artifacts of the Dartmouth group, who appear not to understand that most health care is consumed by a small proportion of the population, and, in urban areas where the concentration of specialists is highest, the high utilizers are disproportionately poor, poorly educated and with poor outcomes. So put together the affluence of urban America with the poverty that dwells within it and suddenly Dartmouth doubletalk is understandable — not too many doctors causing bad outcomes but a inadequate support systems for the nation’s neediest, who look to the health care system (and its doctors) to repair the ills that beset them.
To their credit, some national organizations have stepped forward. Two years ago, the federal government’s Council on Graduate Medical Education, which championed the notion of too many physicians throughout the 1990s, changed its stance and projected future shortages, instead. The Association of American Medical Colleges followed suit a year later, and the American Medical Association soon thereafter. But none of this has translated into a national plan for financing the necessary growth of medical schools and residency training programs. And the clock keeps ticking.
It falls to the public to make its needs known, to proclaim its frustration with waiting times, to protest the indignities that a stressed system showers upon them, to raise concern about the care that they will receive as they age and to express fears about the care that their children and grandchildren will receive. Yet how many among them can even imagine what lies ahead as the available supply of physicians fails to keep up with the needs and the system spirals increasingly out of control. All the more reason that leaders in medicine and government must take it upon themselves to begin the arduous task of developing long-term plans to finance an expansion of medical education so that Americans will have the doctors who they expect and deserve.
MAKE THE US SELF-SUFFICIENT July 2007
Terrifying words emanate from Jordan through Glasgow to London and over the Atlantic to the US. “Those who cure you will kill you.” A band of radical Islamic doctors has attempted heinous crimes. The first question that comes to mind is, how could they? After all, they’re physicians. But underlying that is an even more puzzling question. Why are England and the US so dependent on foreign physicians? While it may be difficult to become energy-sufficient, it should not be difficult to produce enough doctors, yet deepening shortages of physicians are evolving in the US, and no real efforts are being made to ameliorate the problem.
Let me be clear – most foreign physicians are competent and caring, and no one should fear them. Nor should the US close its doors to immigrants. After all, most of us or our parents or grandparents were immigrants. But let me also be clear that being so highly dependent on foreign physicians is not only a problem for the US. It also is a problem for the developing countries from which most come – countries that need them even more than we do.
What must be done? First, the US must build more medical schools. Not the few that are now on the drawing boards, but enough to add 10,000 additional physicians to the workforce annually, more than double the number recommended by the Association of American Medical Colleges and 5-fold the number that are in various stages of planning. Fewer than that will increase our dependence on foreign physicians.
Second, and crucially, the US must build an equivalent number of residency positions, the second phase of medical education, referred to as Graduate Medical Education. But residencies have been frozen at their 1996 levels by a cap on Medicare funding, which is the principal source of support for Graduate Medical Education.
Why are there caps on Graduate Medical Education? Because planners in the 1990s mistakenly thought that the US was producing too many physicians, and many still do, including MedPAC, the committee that advises Medicare. Planners in the 1980s had the same belief, which led to a voluntary cap on medical school places. But residencies expanded in the early 1990s nonetheless, and to make up for too few US medical graduates, the gates were opened to more foreign medical graduates. That’s how the US became so dependent on foreign physicians. Now, residencies must expand again to meet the national need for physicians, but with too few medical schools, the experience of the 1990s will be repeated again.
The simple truth is that there’s a doctor shortage and it’s getting worse. Patients who have tried to get an appointment know it, and so do hospitals and practice groups that have tried to hire an additional doctor. The reason is not complicated. It’s that the US has not built the capacity to train enough new physicians to care for a growing and aging population, one that seeks the technologically-advanced, comprehensive medical care that is possible today. But we can do better. More than 30 state medical societies, hospital associations and medical specialty organizations have called for action. It’s time to remove the caps on Graduate Medical Education and build a sufficient number of medical schools and residency programs to meet the Nation’s needs. Becoming self-sufficient in educating physicians is the responsible thing to do – for the US and for the world.
EXPAND THE PHYSICIAN WORKFORCE April 2009 (Letter)
There clearly is an increasing shortage of primary care physicians. But it isn’t simply because primary care physicians aren’t paid enough, although they aren’t. It is because there are not enough physicians overall. Shortages exist in cardiology, critical care, emergency medicine, general surgery, gastroenterology, nephrology, oncology, orthopedic surgery and radiology, to name just a few. Hospital and medical associations in states encompassing more than half of the US population have warned of deepening shortages, often emphasizing the greater severity in rural areas.
And worse, we can’t even begin to fix the problem, because Medicare, which provides most of the financial support for residencies, capped the number of positions it would support a decade ago. In fact, that’s why we now have shortages. And even worse, no matter what is done today, these shortages cannot be fixed for 15 years or more because it takes too long to build medical schools and residency programs and too long to train physicians. We cannot begin to meet today’s needs with physicians alone.
So our task is two-fold. We have to expand the number of physicians being trained so that our system can function 15-20 years from now, and we have to train and credential more nurse practitioners to do many things that physicians now do, particularly in primary care.
HOW WILL THE SYSTEM OPERATE WITH TOO FEW PHYSICIANS, November 2013 (Letter)
In response to your editorial, The Shame of American Health Care, which cites the Commonwealth Fund’s recent International Profiles of Health Care Systems, it is important to note, as the Commonwealth Fund report did, that the US has fewer physicians per capita than any of the other countries examined, except for Japan. Even including Japan, the number of physicians per capita in the US is 70% of the median of the others. It is little wonder that the US ranks poorly in access and other measures that your editorial cites. We have a physician shortage and it is getting worse daily, on course to reach 150,000 within a decade. Physicians are not the only providers of care, but it is difficult to imagine how our system will function with gross inadequacies in the numbers of physicians available to care for patients.